The industry built AI to process millions of claims. It never built accountability for what they decided.
A strategic proposal on one reframe: making AI decisions legible is not the same as making them accountable. Every structural choice follows from that.
Three events in 2024 made the status quo untenable, and opened a window to lead, not react.
None of it was a messaging problem. Standing still had quietly become the expensive option.
AI auto-denied post-acute claims in 1 to 2 days, regardless of medical necessity.
The window opened to respond structurally, not defensively.
72% of Medicare seniors can't understand their denial letters.
Everyone optimized how the decision feels. Nobody built the layer that makes it auditable.
The whole category competed on the same surface. The accountability layer underneath was open ground.
Aetna, Cigna, and Humana each invested in the front-end experience of a denial: clearer letters, friendlier portals, better scripts. None built the internal layer where a decision can actually be examined.
That layer is organizational and legal, not a feature. It survives cost-cutting because it is written into how the company is accountable to itself, which is why a competitor can’t close it in a quarter.
UnitedHealthcare’s opening: patient transparency and internal compliance on one data layer. The first to build the layer underneath.
Making a denial letter clearer does not make the system more accountable.
Legibility
Accountability
When AI decides whether to cover your MRI, accountability cannot be designed into the interface. It has to be built into the governance structure: the architecture, the org design, and the legal agreements that hold when cost pressure arrives.
Four decisions, one platform built to be audited.
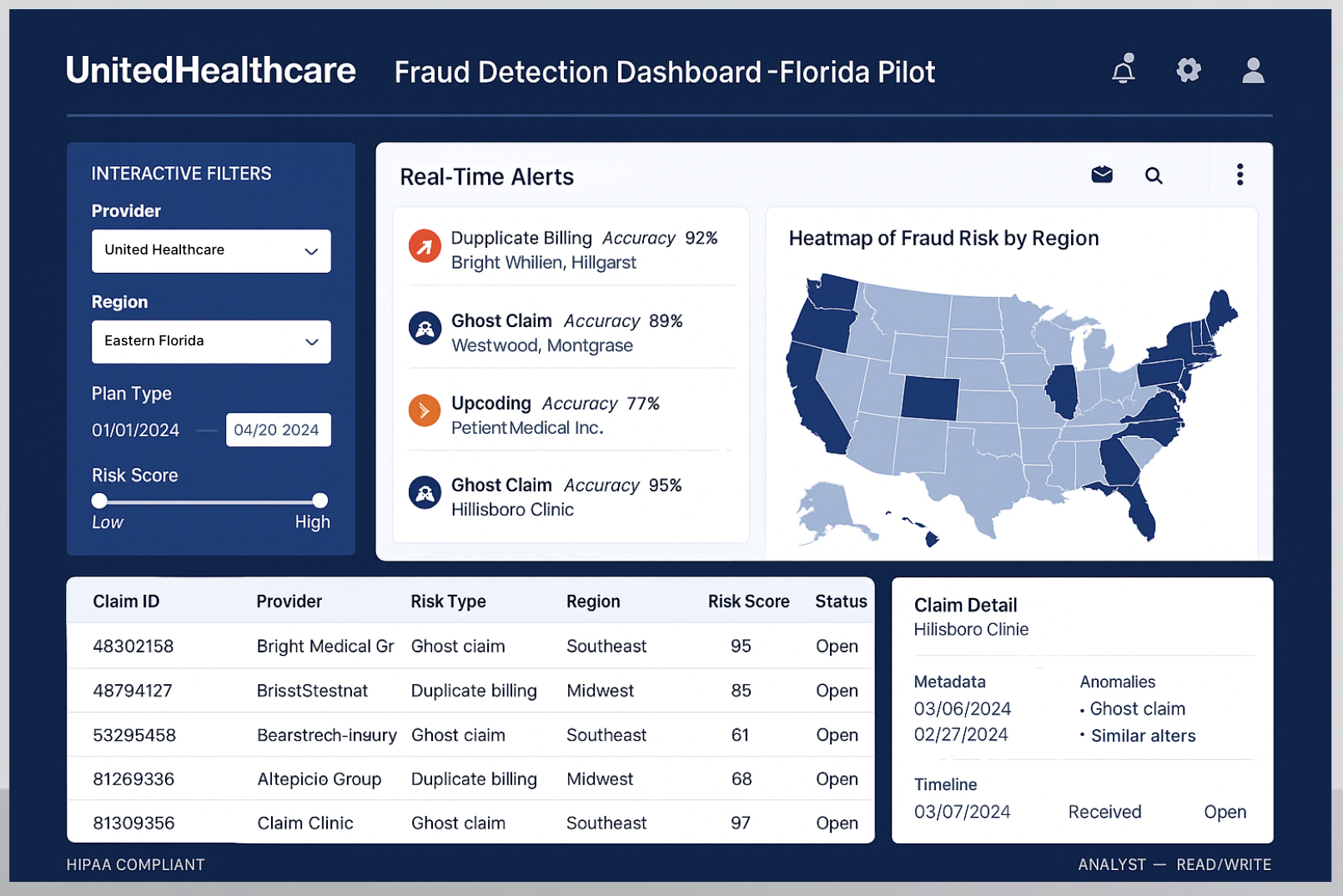
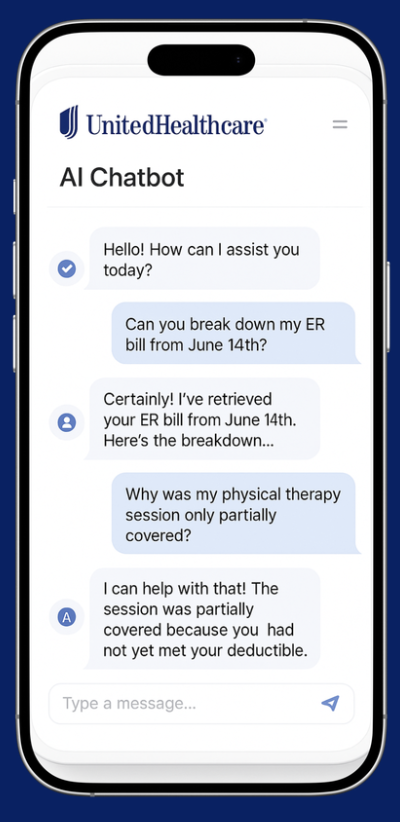
Dual-sidedPatient chatbot and compliance dashboard on one shared data layer.
Patient-facing only Leaves the regulator no way to audit the decision.
Florida21% Medicare, bilingual from day one.
A softer market Only proves the system works when nothing is at stake.
Palantir FoundryHIPAA-native, CDC and UK NHS trusted, modular.
Building in-house Costs 18 to 24 months UHC does not have under scrutiny.
In the contractFour enforceable legal mechanisms, not product guidelines.
Product guidelines Get deferred the first cost-cutting quarter. Contracts don't.
What we consciously gave up.
Dual-sided over patient-only
A validated single-team playbook.
The only position a regulator can't dismiss as a comms fix.
Florida over a softer market
The safety of a clean success story.
A real signal: hold here, hold anywhere.
Palantir over in-house
Full ownership and lower licensing cost.
18 to 24 months faster, with CDC and NHS credibility.
Governance in the contract
Vendor flexibility and a standard timeline.
Accountability that survives a budget cut.
Embedded chatbot
A clean UX free of the legacy portal.
Adoption with no new app to download.
Real implementation starts with the organizational design question, before the technology. This proposal does not go there.
The barrier between patient experience and compliance at UHC’s scale is structural and regulatory, not a communications problem. A stakeholder liaison and sprint demos are not enough, and saying so is part of the work.
The AI was not the risk. The behavior was.
The $4.5M swing between best and worst case is not the AI, the infrastructure, or the contract. It is whether Medicare seniors change how they ask for help.
chatbot adoption, the rate the model actually plans for, between the 15% that loses and the 65% that pays. The whole swing turns on this one behavior.
Did accountability shift, or only the interface?
Projected targets, not outcomes, from the financial model and CMS standards. What the system was designed to reach, and what I’d be held to.
CMS reporting accuracy
Any error recreates the exposure. Everything else is a target; this is the line that cannot move.
Qlarc.
Vendors had the AI governance. Buyers required proof of it. The gap between them was killing deals.